
If you are a provider of adult social care in England, you will be aware that the Care Quality Commission is updating its inspection methodology and the system it uses to inspect and decide on ratings for care services.
In this article we will dive into what is being changed, why and what is staying the same, so that by the end of reading it you and your care service will be as prepared as possible for those changes.
Why are they changing?
Before the pandemic, CQC were clear that they needed a way to look at the quality of care across health and care systems. They knew their regulation needed to be less complex and more efficient and wanted to regulate in a smarter way – being able to adapt and respond to risk, uncertainty and demand, with data and information at their fingertips. The pandemic highlighted the areas that they already knew needed to change.
The regulator wants to have clear, transparent ratings which are current, meaningful and easy to understand for providers and members of the public. They want to use data and insight to help them focus their resources and allow them to spend more time with providers on improvement activities.
They aim to:
- Have greater focus on care across local areas and systems.
- To use their new regulatory powers to effectively improve people’s care.
- To make their regulation less complex and more efficient.
- To regulate in a smarter way.
- To work better with the sector as it changes and recovers.
What’s Changing?
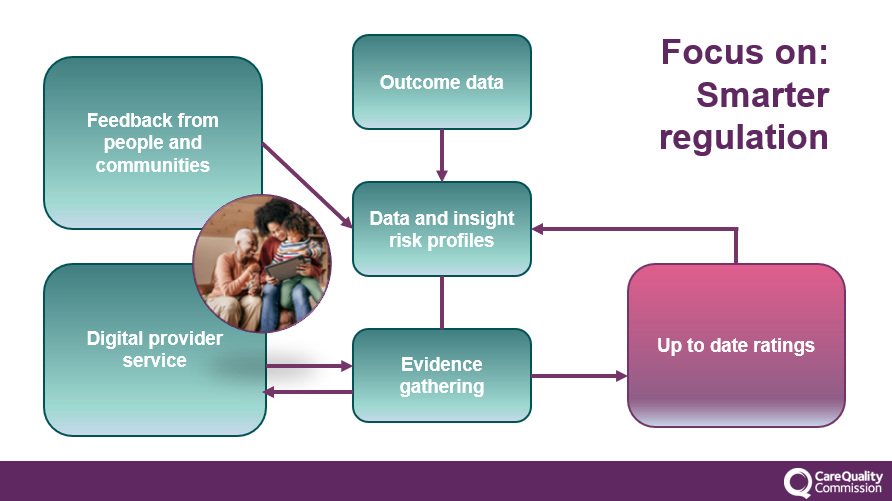
Their new assessment approach means they are moving away from separate ‘monitor,’ ‘inspect’ and ‘rate’ steps. Instead, they will use information from a range of sources to assess providers more frequently and in a more flexible way, without being driven by a previous rating. This is key for them to achieve their strategic ambition of providing an up-to-date view of quality.
New Policy and Powers
The CQC now have new powers to oversee local authorities and integrated care systems under the Health and Care Bill, based on three key themes for assessment: Leadership, Integration and Quality and Safety
The regulator will use a new single quality assessment framework for all service types and at all levels, from registration through to provider assessments and assessments of integrated care systems (ICSs) and local authorities. This will be the basis for their judgements about quality.
Introduction of Quality Statements
Under each of the Key Questions (Safe, Effective, Responsive, Well-Led and Caring) will be new Quality Statements. This change is not about overhauling what the CQC look at in their assessments but instead about streamlining much of the duplication that existed with 120 KLOEs, now into 34 quality statements, with the aim to be clearer to understand for both providers and inspectors.
| Safe | Caring | Responsive | Effective | Well-Led |
| Learning culture | Kindness, compassion and dignity. | Person-centred care. | Assessing needs. | Shared direction and culture. |
| Safe systems, pathways and transitions | Treating people as individuals. | Care provision, integration, and continuity. | Delivering evidence-based care and treatment. | Capable, compassionate and inclusive leaders. |
| Safeguarding | Independence, choice and control. | Providing information. | How staff, teams and services work together. | Freedom to speak up. |
| Involving people to manage risks | Responding to people's immediate needs. | Listening to and involving people. | Supporting people to live healthier lives. | Workforce equality, diversity and inclusion. |
| Safe environments | Workforce wellbeing and enablement. | Equity in access. | Monitoring and improving outcomes. | Governance, management and sustainability. |
| Safe and effective staffing | Equity in experiences and outcomes. | Consent to care and treatment. | Partnerships and communities. | |
| Infection prevention and control | Planning for the future. | Learning, improvement and innovation. | ||
| Medicines optimisation | Environmental sustainability – sustainable development. |
Introduction of Evidence Categories
Under each Quality Statement is evidence categories which vary for different types of services. For example the evidence for care homes is now different to home care.
The six categories are:
- People’s experiences of Health and Care Services -
- Feedback from staff and leaders
- Feedback from partners
- Observation
- Processes
- Outcomes
Each category sets out the types of evidence they use to understand the quality of care being delivered and performance against each quality statement. One common theme is they are focused on outcomes to provide consistency and transparency.
New Ways of Working and Inspecting
Named inspectors are going and they are introducing multidisciplinary teams consisting of inspectors and assessors who specialise in either hospitals, primary care or adult social care. CQC has stated that the relationship will be with the team rather than with an allocated lead inspector.
Alongside this, the way they gather evidence is also changing, with more emphasis on people’s experiences. They will gather evidence to support their judgements in a variety of ways and at different times – not just through inspections. This means inspections will support this activity, rather than being their primary way to collect evidence.
If you are a residential care provider, the CQC will still physically ‘cross your threshold’ to inspect, but they will also gather evidence from you and others at different times and in different ways and these will be called an assessment. Some of these methods will include:
- Providers submitting specific evidence.
- Direct contact with people using the service.
- Structured conversations with managers and other leaders.
- Provider information returns.
- Data already available (skills for care data set, capacity tracker, PAMMS inspections etc)
They will no longer use the rating of a service as the main driver when deciding when they next need to assess. Evidence they collect or information they receive will be assessed against the quality statements and this could trigger the CQC reassessing your quality and safety without always physically inspecting your service. This can lead to changes in one of your key ratings and your overall rating. CQC have stated this is to ensure that there is a continuous and up to date view of the quality and safety of the care people receive.
Factual Accuracy Check
Renamed from the Factual Accuracy Challenge, this process is described as a ‘review and submit further evidence’ and is the route open to providers to challenge the CQC report and ratings. It is based on your ability to provide evidence that either counters the factual basis for the CQC’s judgement or that you believe should be considered. On receipt of the draft report, you have ten days to respond.
New Portal
The CQC have created a new online portal that will be simple and intuitive to enable providers to submit information to them. They want to make it easier for providers to work with them, so they will collect data in a more structured format. They will ask providers to validate the information they hold and ask for the information that they cannot get elsewhere in a way that makes it easy to get right the first time – both for registration and assessment use.
Stay up to date and getting ready.
- Keep checking the CQC website – they won’t necessarily make it obvious what has been updated, but it is being updated on a regular basis. Changes are date stamped on their website though. Find out more here: www.cqc.org.uk/assessment/
- Undertake a mock inspection, this should be done by someone else in your organisation or a third party. Please do not pay for an expensive ‘new single assessment mock inspection’ as no one truly knows what this is going to look like yet. A mock inspection will ensure you are fully compliant with the current CQC’s regulation, help you determine how efficiently your service is and identify where improvements can be made. It can help gain valuable insight and a clear action plan.
- Check out The Caring View who are the leading free resource for social care and have a dedicated CQC Single Assessment Hub full of free templates on their website. Find out more at www.thecaringview.co.uk.
- Review your organisations internal processes to ensure these are aligned with the Quality Statements and the specific Evidence Categories relevant to your service.
- Be proactive in capturing, monitoring and recording your own data and make sure it is organised, analytical and factual. The CQC love to see where you have made a positive impact, so make sure you capture that too.
- Check out W&P Training which are a family run business passionate about supporting Health and Social Care Providers & Local Authorities to improve and develop their services. Find out more here: www.wandptraining.co.uk. I have found their training solution to be flexible and affordable with many of their courses only having to be purchased once, with an unlimited amount of licences to then train your team. They have recently added some dates for their new CQC compliance training for the CQC’s Single Assessment Framework. More information can be found here: https://www.wandptraining.co.uk/cqc-compliance/cqc-compliance-training/improve-webinar/
- Share information with your team to support their understanding of the changes as they emerge. Try to reduce and remove the fear factor of the regulator.
Final thoughts
The new framework may seem daunting but there is a lot of information on then CQC’s website. Remember, the new way of inspecting is not new, and the evidence categories are purely streamlining the 120 key lines of enquiries into 34 easier ones. I have found once you have your head around the Single Assessment Framework, Quality Statements and Evidence Categories the rest really does fall into place.
You can always reach out to me on LinkedIn (www.linkedin.com/in/marktopps/) or via email at thecaringview@gmail.com


